In this module, we will explore key aspects of IBD, including its definition and epidemiology as well as diagnosis, treatment, health maintenance, and preventative care. Additionally, we will highlight the crucial role of patient-provider partnerships, shared decision-making, approaches to patient education and empowerment, and efforts to address social determinants of health (SDOH) and racial disparities in IBD care.
IBD Fundamentals
Topic outline
-
IBD Fundamentals
-
As IBD becomes increasingly prevalent, understanding its impact is more important than ever. This infographic explores changing demographics, key challenges, and opportunities to help advance patient care.

Developed in collaboration with Maia Kayal, MD
Paid consultant for Takeda Pharmaceuticals.Collaborator
Maia Kayal, MD
Read time
5:00 minutes
Learn more-
Students mustMark as done
As IBD becomes increasingly prevalent, understanding its impact is more important than ever.1
Explore the changing demographics, key challenges, and opportunities to help advance patient care.
Epidemiological stages of IBD evolution1
Stage 1
Emerging Incidence
What:
Sporadic cases begin to appearWhere:
Developing countriesStage 2
Accelerating Incidence
What:
Incidence increases, prevalence remains lowWhere:
Newly industrialized countriesStage 3
Compounding Prevalence
What:
Incidence stabilizes, prevalence rises sharplyWhere:
Western nationsStage 4
Prevalence Equilibrium
What:
Growth in prevalence levels off as new cases are offset by an aging populationWhere:
Predicted to begin in Western nations ~2050 -
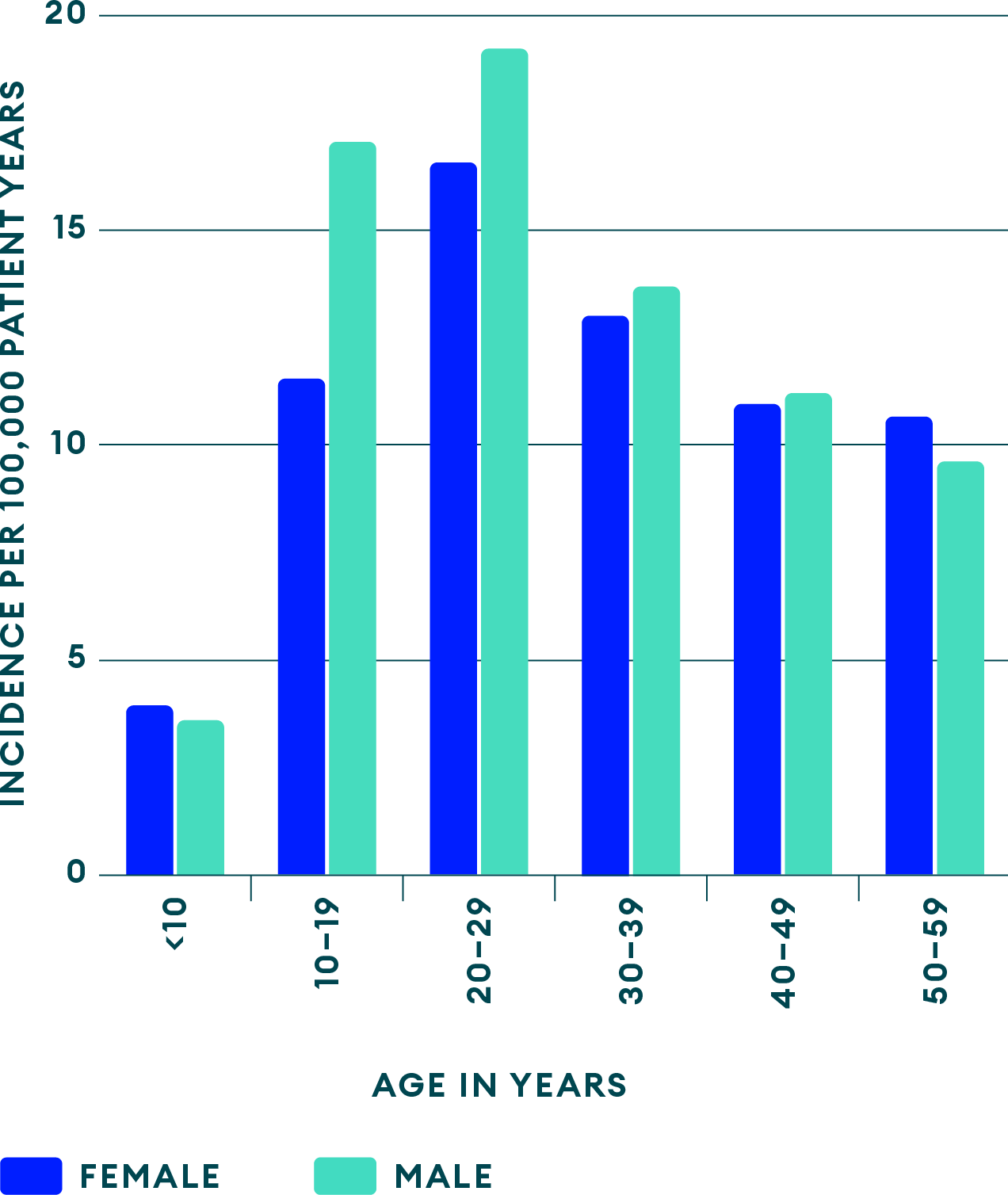
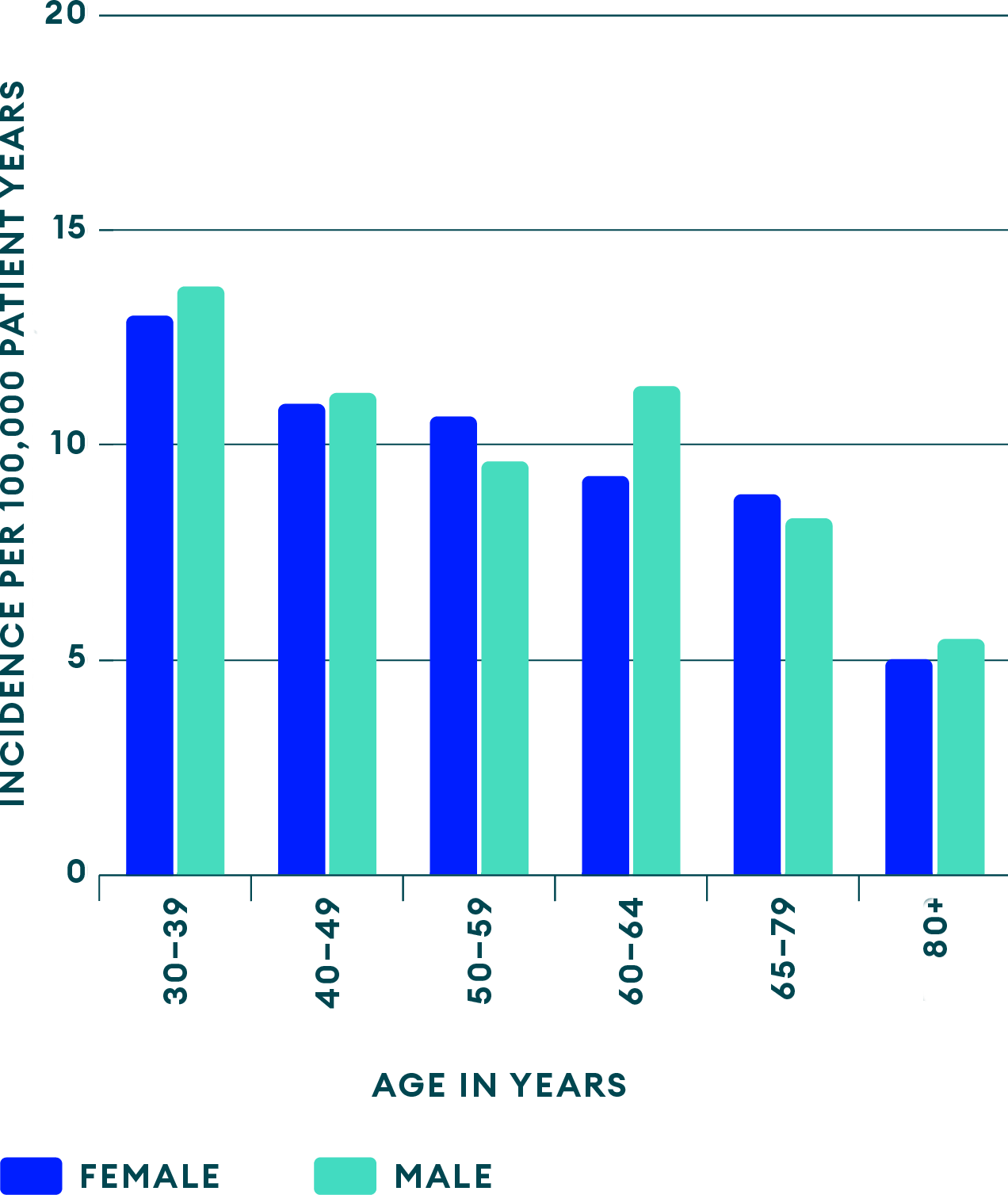
IBD incidence by age group in the US3,5
Peak age of onset Average age at diagnosis Decline to stable levelMost often ages 31–34

-
Factors associated with the pathogenesis of IBD
Combination of contributing factors6

Genetics

Altered Gut
Microbiome
Dysregulated
Immune
Responses
Environmental
Risk FactorsKey environmental
risk factors2
Antibiotics

Select
Infections
Combined Oral Contraceptives

Tobacco
Smoking
Ultra-High Processed
Foods
Western and
Carnivorous
Diet -
Approaches to help improve IBD care

Early diagnosis and risk stratification
Elevate HCP awareness of signs and symptoms, and access to specialists/prognostic tools14

Cost-effective care
Leverage telemedicine, noninvasive biomarkers, biosimilars when appropriate, top-down initiatives, and the promotion of healthy living15

Multidisciplinary models
Integrate dietary therapy, psychological care, and various support strategies15
-






