Anti-TNFs
Anti-TNFs
Anti-TNFs
Information included in this Introduction to IBD Medication Classes is for educational purposes only and is intended for US-based healthcare providers (HCPs).
This information does not represent medical advice or endorse any specific product. It should not be the basis for clinical diagnoses or treatment decisions.
Use this information in conjunction with a clinical assessment and independent research from other relevant sources.
This information was last updated 12/2025.
Medication Class Introduction
Anti-tumor necrosis factor (TNF) medications are a class of biologics introduced in the 1990s that are used in the treatment of inflammatory bowel disease (IBD) in appropriate patients.1 They are monoclonal antibodies that target and inhibit the TNF-α cytokine, a protein involved in the gastrointestinal tract inflammatory process.2 TNF-α plays a key role in the immune response and pathogenesis of IBD.
Biosimilars are monoclonal antibodies that have highly similar clinical characteristics to an FDA-approved reference product.3 There are anti-TNF biosimilars available on the US market.
IBD Treatment Landscape1,4–13
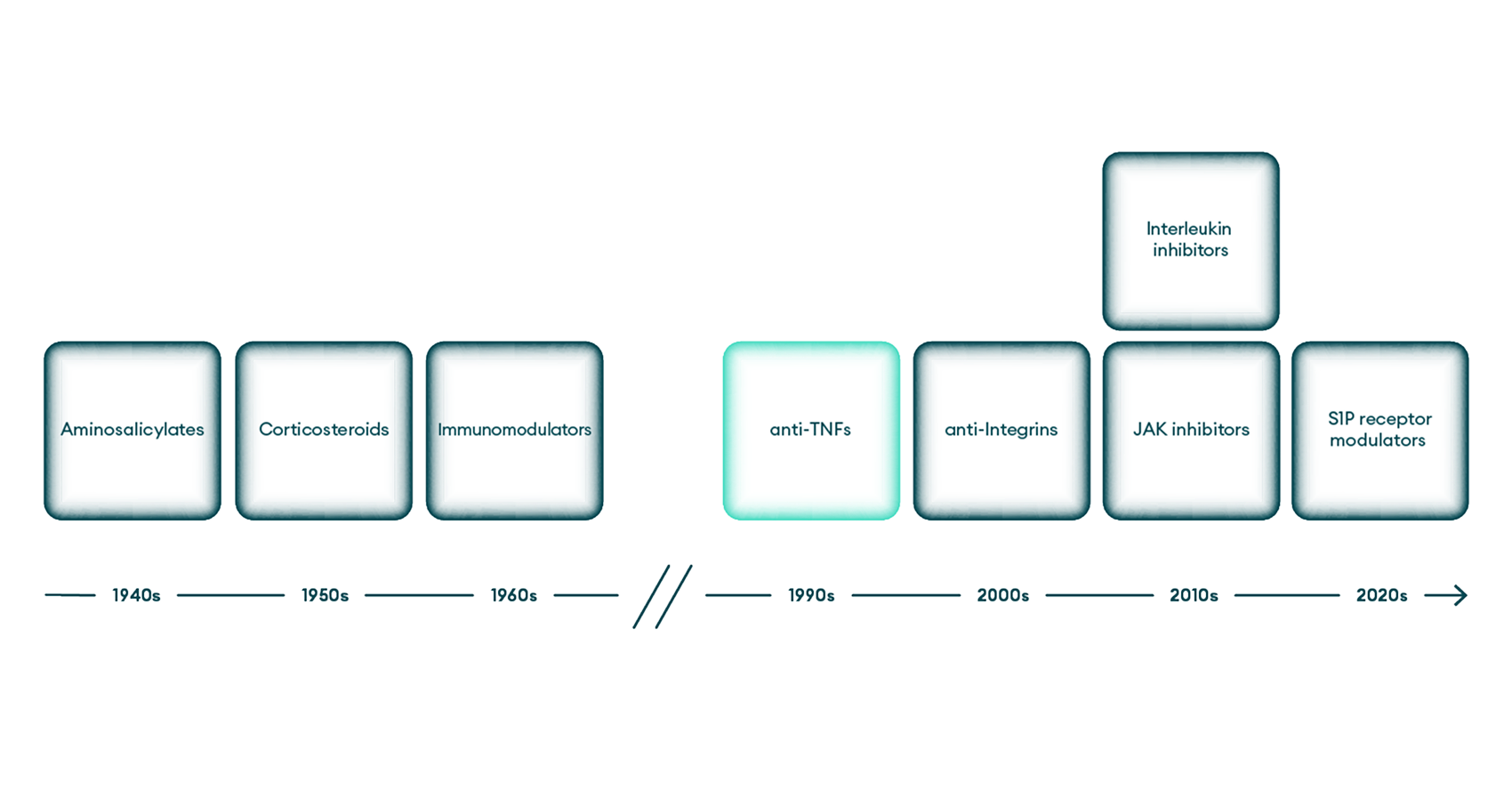
JAK=Janus kinase; S1P=sphingosine-1-phosphate; TNF=tumor necrosis factor.
Role in IBD Pathogenesis
TNF-α levels may be elevated in patients with IBD.2 TNF-α binds to 2 types of receptors: TNF receptor 1 (TNFR1) and TNF receptor 2 (TNFR2).2,14 Once bound to these receptors, TNF-α activates intracellular signaling pathways, inducing expression of pro-inflammatory cytokines. Increased production of these pro-inflammatory cytokines is associated with the inflammatory response that occurs in IBD.2
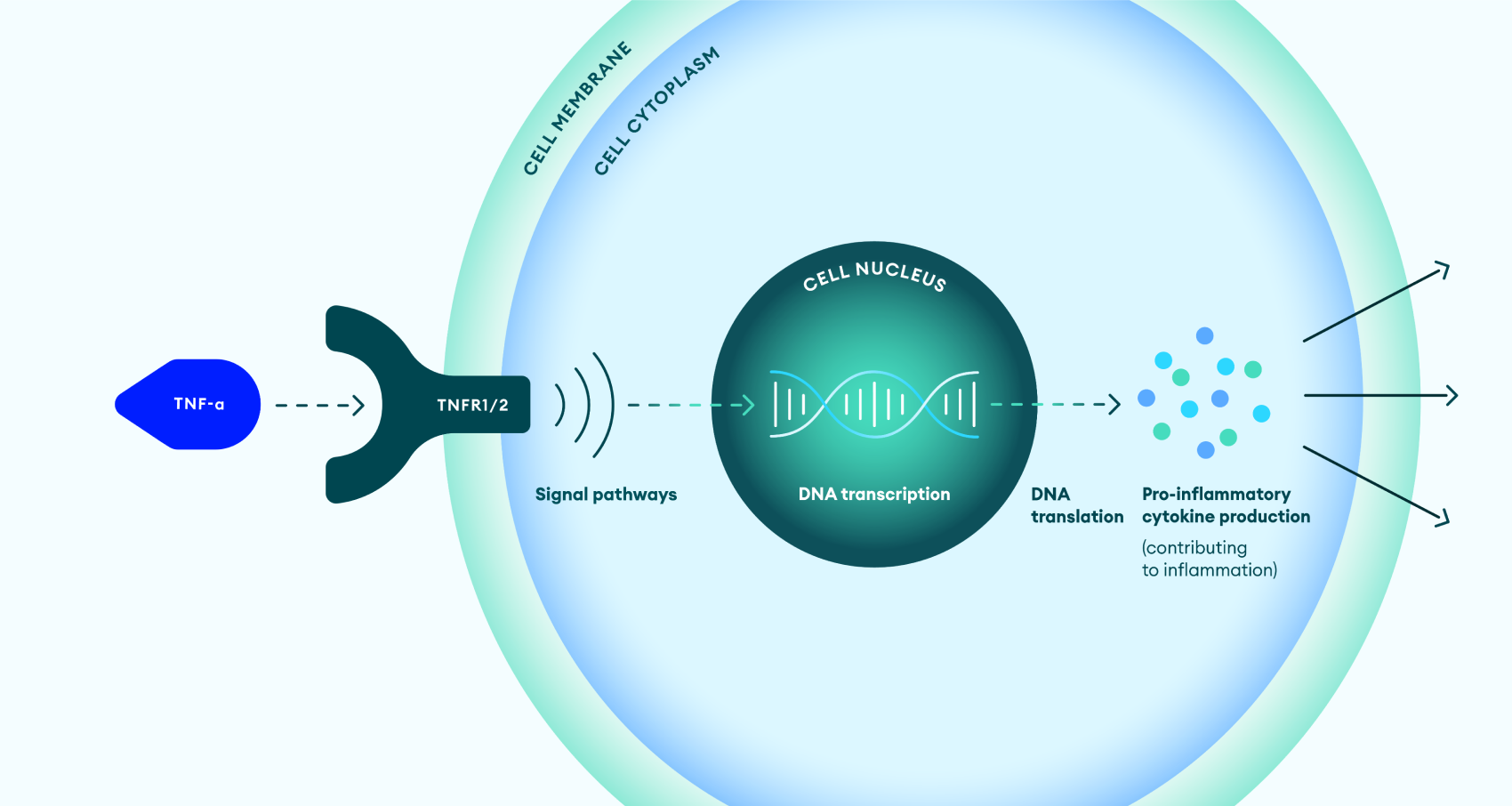
DNA=deoxyribonucleic acid; TNF-α=tumor necrosis factor alpha; TNFR1/2=tumor necrosis factor receptor 1 or 2.
Mechanism of Action in IBD
Anti-TNF medications are monoclonal antibodies that bind to TNF-α and prevent binding to TNFR1 and TNFR2, which inhibits activation of intracellular signaling pathways.2,14,15 This results in decreased levels of the pro-inflammatory cytokines that cause inflammation in the intestines in patients with IBD.2,14,15
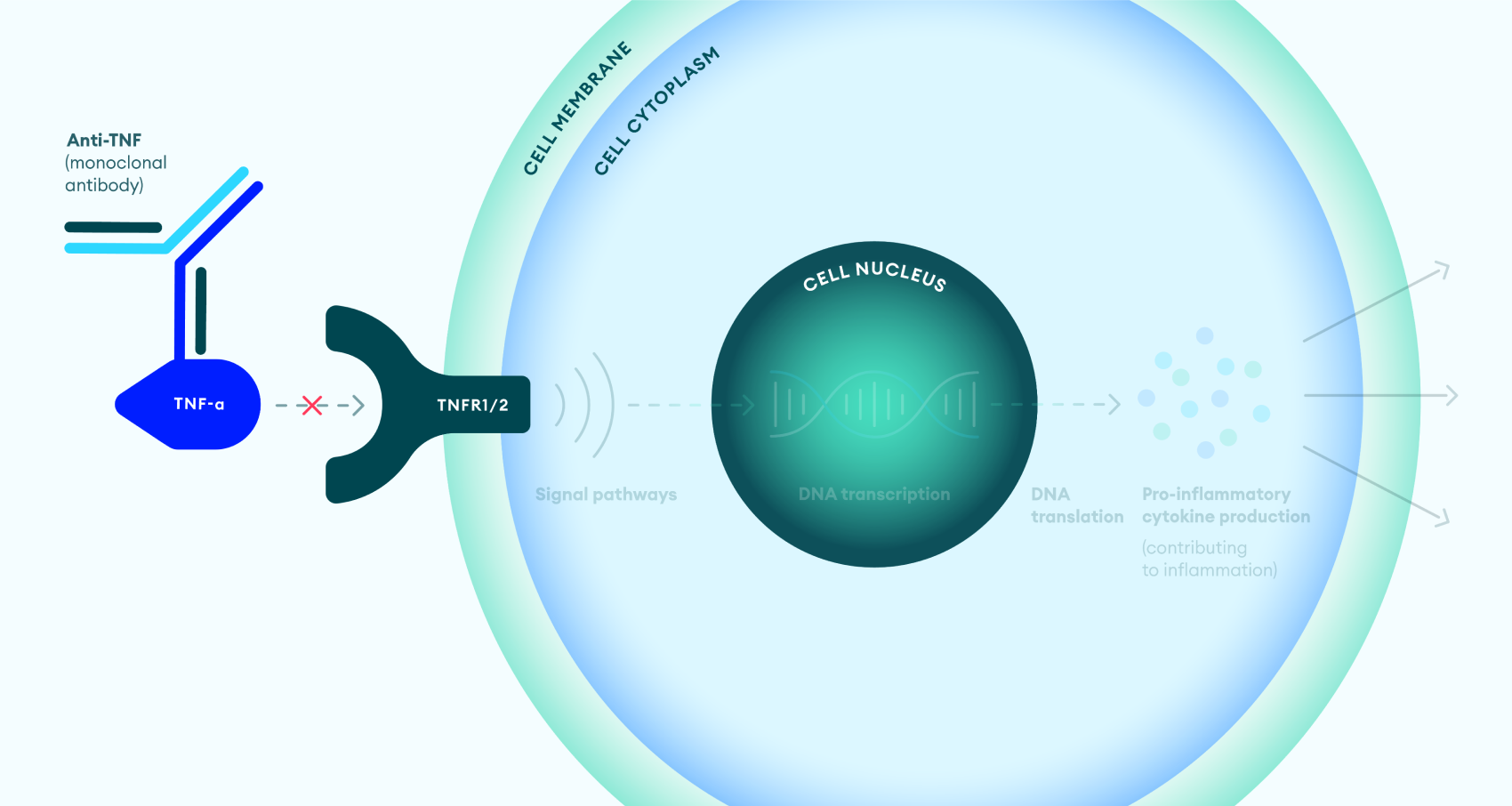
DNA=deoxyribonucleic acid; TNF-α=tumor necrosis factor alpha; TNFR1/2=tumor necrosis factor receptor 1 or 2.
Resources
Current IBD Treatment Guidelines
Guidelines for managing IBD are available from the American College of Gastroenterology (ACG) and the American Gastroenterological Association (AGA). You can access them through the following links:
- ACG Clinical Guideline: Management of Crohn’s Disease in Adults
- ACG Clinical Guideline Update: Ulcerative Colitis in Adults
- AGA Living Clinical Practice Guideline on the Pharmacologic Management of Moderate-to-Severe Crohn’s Disease
- AGA Clinical Practice Guidelines on the Management of Mild-to-Moderate Ulcerative Colitis
- AGA Living Clinical Practice Guideline on Pharmacological Management of Moderate-to-Severe Ulcerative Colitis
Resources to Help Explain Medication Options for IBD to Patients
The Crohn’s & Colitis Foundation resources below may help you explain medication options, including the mechanism of action of IBD medication classes and how they are designed to work in the body, to your patients with IBD.
Resources to Help Understand Medical Management of IBD From UpToDate®
The UpToDate® resources below may help you understand medical management of IBD in adults including but not limited to disease activity, severity, and risk, as well as medication options for induction and maintenance.
- Medical management of mild Crohn’s disease
- Medical management of moderate to severe Crohn’s disease
- Medical management of mild to moderate ulcerative colitis
- Medical management of moderate to severe ulcerative colitis
For More Information on IBD Medications
To learn more about the medications commonly used to treat IBD—including potential side effects and safety considerations—please refer to the following resource:
Links to third-party websites are provided as resources and not intended to be an endorsement. Takeda is not responsible for their content.
- Actis GC, Pellicano R, Fagoonee S, Ribaldone DG. J Clin Med. 2019;8(11):1970.
- Souza RF, Caetano MAF, Magalhães HIR, Castelucci P. World J Gastroenterol. 2023;29(18):2733-2746.
- Angyal A, Bhat S. Curr Gastroenterol Rep. 2024;26(3):77-85.
- Murray A, Nguyen TM, Parker CE, Feagan BG, MacDonald JK. Cochrane Database Syst Rev. 2020;8(8):CD000544.
- Dorrington AM, Selinger CP, Parkes GC, Smith M, Pollok RC, Raine T. J Crohns Colitis. 2020;14(9):1316-1329.
- de Boer NKH, Peyrin-Biroulet L, Jharap B, et al. J Crohns Colitis. 2018;12(5):610-620.
- Lichtenstein GR, Loftus EV, Afzali A, et al. Am J Gastroenterol. 2025;120(6):1225-1264.
- Santiago P, Braga-Neto MB, Loftus EV Jr. Gastroenterol Hepatol (N Y). 2022;18(8):453-465.
- Pérez-Jeldres T, Tyler CJ, Boyer JD, et al. Front Pharmacol. 2019;10:212.
- Fudman DI, McConnell RA, Ha C, Singh S. Clin Gastroenterol Hepatol. 2025;23(3):454-469.
- Moschen AR, Tilg H, Raine T. Nat Rev Gastroenterol Hepatol. 2019;16(3):185-196.
- Choden T, Cohen NA, Rubin DT. Gastroenterol Hepatol (N Y). 2022;18(5):265-271.
- Martinez-Molina C, González-Suárez B. J Clin Med. 2025;14(11):3890.
- Pedersen J, Coskun M, Soendergaard C, Salem M, Nielsen OH. World J Gastroenterol. 2014;20(1):64-77.
- Nielsen OH, Ainsworth MA. N Engl J Med. 2013;369(8):754-762.
US-NON-10456v1.0 12/25